Bacterial Sepsis in Pregnancy Green top Guideline No. 64a April 2012-
Summary and Discussion
Severe sepsis with acute organ dysfunction has a mortality rate of 20 to 40%.
Septic Shock has a mortality rate of 60%.
Early recognition and initiation of treatment can improve survival rates.
Disease progression may be much more rapid in pregnant patients.
The scope of the guideline covers the recognition and management of serious
bacterial illness in the antenatal and intrapartum periods, arising in the genital tract or elsewhere, and its management in secondary care.
Definitions-
Sepsis may be defined as infection plus systemic manifestations of infection.
Severe sepsis may be defined as sepsis plus sepsis-induced organ dysfunction or tissue hypoperfusion.
Septic shock is defined as the persistence of hypoperfusion despite adequate fluid replacement therapy.
Risk factors for maternal sepsis in pregnancy-
Urinary Tract Infection
Chorioamnionitis
Obesity
Impaired glucose tolerance / diabetes
Impaired immunity/ immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal infection
Amniocentesis and other invasive procedures
Cervical cerclage
Prolonged spontaneous rupture of membranes
GAS ( Group A Streptococcus) infection in close contacts / family members
Black or other minority ethnic group origin
Recognition of Sepsis
In a pregnant woman, Signs and Symptoms of Sepsis may be less distinctive.
Also the signs and symptoms are not necessarily present in all cases. Therefore, a high index of suspicion is necessary.
All clinicians should be aware of the symptoms and signs of maternal sepsis and critical illness and of the rapid, potentially lethal course of severe sepsis and septic shock.
Suspicion of significant sepsis should trigger an urgent referral to secondary care.
Remember- SEPSIS & SEPTIC SHOCK ARE MEDICAL EMERGENCIES.
Regular observations of all vital signs (including temperature, pulse rate, blood pressure and
respiratory rate) should be recorded on a Modified Early Obstetric Warning Score (MEOWS) chart.
( A MEOWS chart should be used for all maternity inpatients to aid early identification of seriously ill patients) .
Clinical features suggestive of sepsis –
- Fever or rigors
- Diarrhoea or vomiting – may indicate exotoxin production (early toxic shock)
- Rash (generalised streptococcal maculopapular rash or purpura fulminans)
- Abdominal /pelvic pain and tenderness
- Offensive vaginal discharge (smelly suggests anaerobes; serosanguinous suggests streptococcal infection)
- Productive cough
- Urinary symptoms
Actions to be taken when sepsis is suspected–
1.Act quickly upon sepsis & septic shock recognition
2. Minimize time to treatment – sepsis & septic shock are medical emergencies
3. Monitor closely for response to interventions
4. Communicate sepsis status in hand-offs.
The GTG 64 a was developed in 2012 and mentions initiating a resuscitation bundle within 6 hours .( Quoting the Surviving Sepsis Campaign Guidance from 2008) . The fourth edition of “Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock was released in 2016 , and mentions an ’ Hour 1 Bundle ‘ which should be within one hour upon recognition of sepsis/septic shock.
The pdf of the Surviving Sepsis Campaign Hour1 Bundle can be accessed here- https://www.sccm.org/getattachment/SurvivingSepsisCampaign/Guidelines/Adult-Patients/Surviving-Sepsis-Campaign-Hour-1-Bundle.pdf?lang=en-US
IF SEPSIS IS SUSPECTED-
- – Perform regular , frequent observations
- – Involvement of a consultant obstetrician
- – In severe or rapidly deteriorating cases- Urgent referral to the critical care team + advice of a consultant microbiologist or infectious disease physician.
HOUR-1 BUNDLE: INITIAL RESUSCITATION FOR SEPSIS AND SEPTIC SHOCK ( Should be done before shifting to ICU or other center)
1) Measure lactate level. *
2) Obtain blood cultures before administering antibiotics.
3) Administer broad-spectrum antibiotics.( recommended within one hour of suspicion of severe sepsis, with or without septic shock ) .
4) Begin rapid administration of 30mL/kg crystalloid for hypotension or lactate ≥4 mmol/L.
5) Apply vasopressors if hypotensive during or after fluid resuscitation to maintain a mean arterial pressure ≥ 65 mm Hg.
*Remeasure lactate if initial lactate elevated (> 2 mmol/L)
Appropriate swabs depending on the clinical situation should be sent.
Nasal swabs for Methicillin Resistant Staphylococcus Aureus can be sent for rapid screening( if such screening is available)
The lab results should be reviewed periodically to guide treatment.
Prompt imaging may also be used to look for source of infection.
The diagnostic criteria for sepsis ( Copied from the GTG) are as follows and can be seen in the Appendix 1 of the GTG( https://www.rcog.org.uk/globalassets/documents/guidelines/gtg_64a.pdf ).
The variables measured in diagnosis of Sepsis can be categorized into –
1. General variables 2. Inflammatory variables 3. Haemodynamic Variables
4. Tissue Perfusion Variables and 5. Organ dysfunction Variables.
A diagnosis of sepsis is defined as Infection( documented or suspected) , and some of the following:
- General variables:
Fever (>38ºC)
Hypothermia (core temperature <36ºC)
Tachycardia (>100 beats per minute)
Tachypnoea (>20 breaths per minute)
Impaired mental state
Significant oedema or positive fluid balance (>20ml/kg over 24 hours)
Hyperglycaemia in the absence of diabetes (plasma glucose >7.7 mmol/l)
- Inflammatory variables:
White blood cell (WBC) count >12 x 109/l (note that a transient leucocytosis is common in labour)
Leucopenia (WBC count <4 x 109/l)
Normal WBC count with >10% immature forms
Plasma C-reactive protein >7mg/l
- Haemodynamic variables:
Arterial hypotension (systolic blood pressure <90mmHg; mean arterial pressure <70mmHg or systolic blood pressure decrease >40mmHg)
- Tissue perfusion variables:
Raised serum lactate ≥ 4 mmol/l
Decreased capillary refill or mottling
- Organ dysfunction variables:
Arterial hypoxaemia (PaO2 (arterial oxygen partial pressure) /FIO2 (fraction of inspired oxygen) <40kPa). Sepsis is severe if <33.3kPa in the absence of pneumonia or <26.7kPa in the presence of pneumonia.
Oliguria (urine output <0.5ml/kg/hr for at least two hours, despite adequate fluid resuscitation)
Creatinine rise of >44.2μmol/l. Sepsis is severe if creatinine level >176μmol/l
Coagulation abnormalities (International Normalised Ratio [INR] >1.5 or activated partial thromboplastin time [APTT] >60s)
Thrombocytopaenia (platelet count <100 x 109/l)
Hyperbilirubinaemia (plasma total bilirubin> 70μmol/l)
Ileus (absent bowel sounds)
The Surviving Sepsis Campaign website has some very useful checklists and protocols which can be easily adapted.
https://www.sccm.org/SurvivingSepsisCampaign/Resources/Protocols-and-Checklists
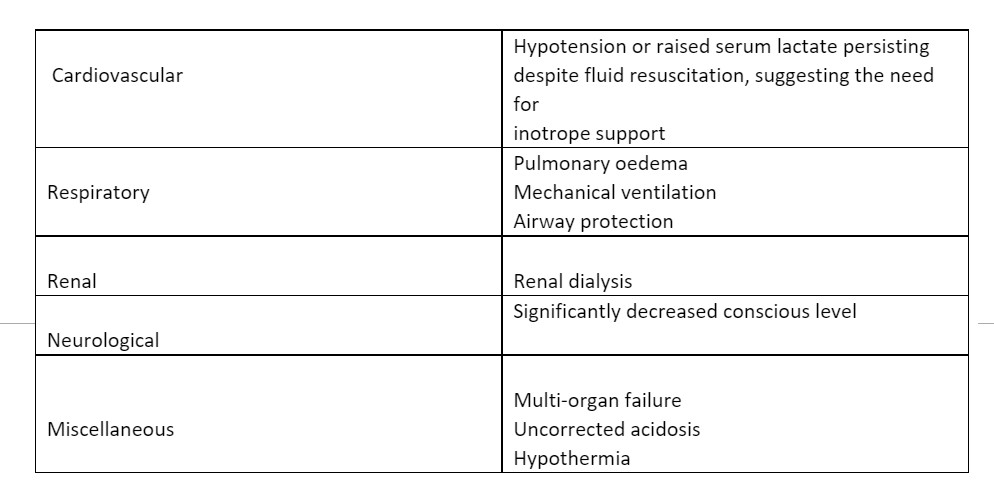
The decision to transfer to the ICU should be taken by an obstetric consultant, consultant obstetric anaesthetist, and the ICU team.
The GTG mentions criteria for ICU care as follows-
Common organisms-
Though the relative prevalence of organisms varies from place to place, according to this GTG-
- The most common organisms identified in pregnant women dying from sepsis are-
Lancefield group A beta-haemolytic Streptococcus and E.Coli.
- In chorioamnionitis- Mixed infections with both Gram-positive and Gram-negative organisms are common.
- In urinary sepsis, preterm premature rupture of membranes, and cerclage- Coliforms are common.
Antibiotics to be used-
Broad spectrum antimicrobials active against Gram-negative bacteria, and capable of preventing exotoxin production from Gram-positive bacteria, should be used according to local microbiology policy.
The therapy can be narrowed once the causative organism has been identified.
Hospital guidelines differ, and local guidance should be followed.
The source of sepsis should be sought and dealt with if possible.
ROLE OF IV Ig
IVIG is recommended for severe invasive streptococcal or staphylococcal infection if other therapies
have failed.
High dose IVIG has been used in pregnant women and is effective in exotoxic shock (i.e. toxic
shock due to streptococci and staphylococci)
There is little evidence of benefit in IV Ig Gram-negative (endotoxin related) sepsis.
The main contraindication to IVIG use is a congenital deficiency of immunoglobulin A.
Administration of IVIg should be administered by a blood warming device.
Considerations around labor and delivery-
The risk of neonatal encephalopathy and cerebral palsy is increased in the presence of intrauterine infection
The fetus may be affected in the following ways
– direct effect of infection
– the effect of maternal illness/shock
-effect of maternal treatment.
– preterm delivery ( preterm labor or induced labor to treat the condition)
The NICE Guideline on intrapartum Care ( Intrapartum care for healthy
women and babies- December 2014 ) mentions that continuous electronic fetal monitoring is recommended in the presence of maternal pyrexia defined as a temperature >38.0 °C once, or 37.5 °C on two occasions 1 hours apart. ( The GTG cites the old , 2007 NICE guideline and defines maternal pyrexia as temperature >38.0 °C once, or 37.5 °C on two occasions
2 hours apart. ) The GTG mentions that Continuous CTG should be done in the presence of maternal pyrexia as well as sepsis without pyrexia.
Objective evidence of intrauterine infection is associated with abnormal fetal heart monitoring.
But electronic fetal monitoring is not a sensitive predictor of early onset neonatal sepsis.
If on CTG, there is change in baseline variability , or new onset decelerations-
1 . Follow the guideline for intrapartum fetal monitoring, But also re-evaluate the mother- mean arterial pressure, hypoxia and acidaemia. CTG Changes may be early warning sign for derangements in maternal end-organ systems.
If preterm delivery is anticipated , the use of antenatal corticosteroids can be considered.
The GTG guideline states that there is insufficient evidence regarding fetal blood sampling in the presence of maternal sepsis to guide practice.
The NICEGuideline CG 190 specifically mentions as follows-
Be aware that for women with sepsis or significant meconium, fetal blood sample results may be falsely reassuring, and always discuss with a consultant obstetrician:
- whether fetal blood sampling is appropriate.
- any results from the procedure if carried out.
Mode and time of delivery
– decision should be individualized. Attempting delivery in the setting of maternal instability increases the maternal and fetal mortality rates unless the source of infection is intrauterine.
Prophylaxis for contacts of mother with sepsis – Follow the local/national guideline
Inform neonatologist- prophylactic antibiotic may be considered.
Specific recommendations if the mother had invasive Group A Streptococcus infection-
- If the infection was during peripartum period- Inform neonatologist, prophylactic antibiotics to be given to the baby.
- Close household contacts of the woman should be warned to seek medical attention if symptoms develop. Consider antibiotic prophylaxis.
- Healthcare workers exposed to Respiratory secretions of the woman- consider antibiotic prophylaxis.
Infection control practices to be followed-
Invasive group A streptococcal infections are notifiable.
The woman should be cared for in an isolated room.
Follow local infection control protocols and involve the infection control team.
The Society of Critical Care Medicine , in 2016 released new definitions for sepsis and septic shock, which can be found here https://www.sccm.org/Research/Quality/Sepsis-Definitions
Sepsis Six Checklist – https://sepsistrust.org/wp-content/uploads/2018/06/ED-adult-NICE-Final-1107.pdf