
The Management of Ovarian Hyperstimulation Syndrome ( OHSS) – Subfertility, Early Pregnancy
Summary of Green-top Guideline No. 5
OHSS is a complication of fertility treatment ( pharmacological ovarian stimulation to increase the number of oocytes) .
Types of OHSS-
Early OHSS – usually presents within 7 days of the hCG injection- usually associated with an excessive ovarian response.
Late OHSS- usually presents 10 or more days after the hCG injection – usually the result of endogenous hCG derived from an early pregnancy- tends to be more prolonged and severe than the early form- in these women, the ovarian response before the pregnancy may be unremarkable.
INCIDENCE– Exact incidence not known ( due to lack of mandatory reporting of mild cases and also due to lack of an internationally recognized classification system) . It is the commonest complication of IVF treatment. Different studies have shown the incidence to be between 1.1 % to 8.9%. The Patient information leaflet by RCOG mentions that of women undergoing IVF, mild OHSS is found in about 33% , while severe OHSS occurs in about just over 1%.
Rarely seen after clomiphene stimulation, very rare after spontaneous pregnancy.
Risk factors for OHSS-
1. Previous history of OHSS
2. Polycystic ovary syndrome
3. Increased antral follicle count (AFC) or high levels of anti-Müllerian hormone (AMH)
4. GnRH agonist use for ovarian stimulation( as compared to GnRH antagonists) .
5. Higher in IVF Cycles which result in pregnancy, and higher in cycles resulting in multiple pregnancy ( as compared to cycles which do not result in conception).
Risks– physical and psychological morbidity, risk of maternal death. Rarely, it may be associated with life-threatening complications, including renal failure, acute respiratory distress syndrome (ARDS), haemorrhage from ovarian rupture, and thromboembolism.
Self limiting condition in most casess.( Resolves over 7 to 10 days in most women) . If conception occurs, endogenous hCG can lead to worsening.
If pregnancy does not occur, recovery is usually complete by the time of the withdrawal bleed.
Main principles of management– early recognition , prompt assessment , treatment of women with moderate or severe OHSS.
Pathophysiology– Controlled Ovarian Stimulation by FSHà Exposure of the stimulated ovaries to hCG or LHà Release of proinflammatory mediators( Mainly VEGF) à Ovarian enlargement + increased vascular permeability and prothrombotic effect à clinical features of OHSS.
Increased vascular permeability à Loss of fluid into third space( Ascites, pleural effusion), reduced serum osmolality and sodium.
Diagnosis is based on clinical criteria. ( The typical patient presents with abdominal distension and discomfort following the trigger injection used to promote final follicular maturation prior to oocyte retrieval) . The combination of elevated haematocrit and reduced serum osmolality and sodium is indicative of OHSS.
History-
· When she received the trigger injection, and when did the symptoms start( to differentiate between early and late OHSS) .
· Medication used for trigger (hCG or GnRH agonist).
· Number of follicles on final monitoring scan, Number of eggs collected, Any embryo transfer done ( and how many).
· Polycystic ovary syndrome diagnosis?
· Symptoms– Abdominal – bloating, discomfort/pain, need for analgesia.
· Nausea and vomiting
· Breathlessness, inability to lie flat or talk in full sentences
· Reduced urine output
· Swelling- Leg , vulva or over sacrum
· Associated comorbidities such as thrombosis
( If there is abdominal pain, shortness of breath, or subjective sensation of reduced urine output, she should have a face to face clinical review- these symptoms may indicate severe OHSS. However , absence of these symptoms does not mean that a face to face review is not required).
Examination and investigation
General examination-
· Heart rate, respiratory rate, blood pressure, body weight
· Dehydration, oedema (pedal, vulval and sacral)
Abdominal – ascites, palpable mass, peritonism; measure girth.
Respiratory- for pleural effusion, pneumonia, pulmonary oedema.
OHSS by itself is not commonly associated with severe pain, pyrexia or signs of peritonism. ( if such symptoms are present, then a thorough evaluation should be done)
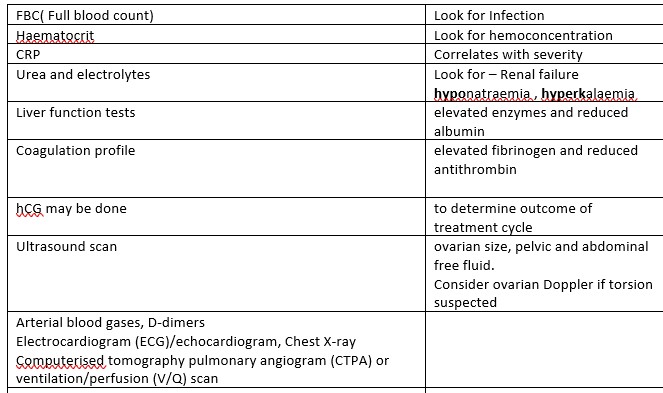
Investigations-
TABLE A
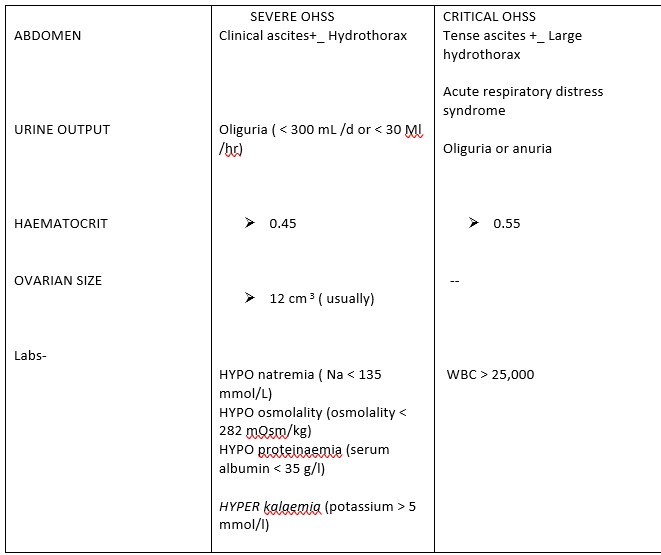
Classification of OHSS- based on severity.

REPORTING of OHSS- As per UK law
Licensed centers – should comply with relevant Human Fertilisation and Embryology Authority (HFEA) regulations in reporting cases of severe or critical OHSS among their patients. The incident should be reported verbally within 12 working hours, followed by a completed incident form within 24 working hours of the incident being identified.
If a patient is going to another center for treatment of OHSS, this treating center should inform the fertility center where the treatment was carried out- and the fertility center should report it.
Any death from OHSS ( regardless of whether the woman was pregnant) – must be reported to MBRRACE-UK.
Advice to patients undergoing fertility treatment– verbal and written information concerning OHSS , and a 24-hour contact telephone number should be given.
They should be advised to mention that they are undergoing fertility treatment even if they present to another hospital or with an apparently unrelated symptom, such as headache or visual disturbance.
INITIAL ASSESSMENT is Done to establish the diagnosis and the grade of severity. The management is then decided according to the severity.
MANAGEMENT-
Outpatient management – Can be done in selected cases.
– Baseline labs to be done
– Counseling and information (verbal and written)
– Contact details on which they can seek information and advice.
– Drink to thirst , maintain fluid intake of at least 1000 ml
– It is better if she can maintain fluid balance chart(If Urine output is < 1000 mL in 24 hours, OR there is Positive fluid balance of more than 1000 mL in 24 hours, then a medical review should be done to assess the severity) .
– For pain relief- Paracetamol and oral opiates. Avoid NSAIDs ( may compromise renal function)
– Severe OHSS being managed as outpatient- Give thromboprophylaxis( Compression stockings, LMWH, advice to move about)
Paracentesis can also be done on outpatient basis ( abdominal or transvaginal) .
Dopamine agonists may have a beneficial role in OHSS. ( More research needed)
Monitoring on outpatient basis– Done to identify women who may be worsening.
Review every 2-3 days.
Specifically look for –
- increasing abdominal distension and pain
- shortness of breath
- tachycardia or hypotension,
- reduced urine output or positive fluid balance ,
- weight gain and increased abdominal girth,
- increasing haematocrit (greater than 0.45).
Baseline labs can be repeated if the OHSS seems to be worsening.
( Haematocrit is a useful parameter to guide about intravascular volume depletion) .
Inpatient management– there are no clear cut criteria for inpatient monitoring. Decision to admit may depend on the social factors, severity of the condition, the facilities available in the hospital , need for closer monitoring etc.
However admission should be considered if the woman is
- unable to achieve satisfactory pain control
- unable to maintain adequate fluid intake due to nausea
- showing signs of worsening OHSS despite outpatient intervention
- unable to attend for regular outpatient follow-up
- has critical OHSS
Care of women with OHSS as inpatient- Multidisciplinary team input for critical OHSS or for Severe OHSS with persistent hemoconcentration and dehydration.
A clinician experienced in management of OHSS should be in overall charge of her care.
Seek advice from Anesthesia /Critical care if –
1. severe OHSS where dehydration and haemoconcentration persist despite adequate fluid replacement ( may need invasive haemodynamic monitoring) , or
2. critical OHSS.
Seek advice from other specialties – if any complications ( Like thromboembolism, ARDS, Renal failure) .
Monitoring of Inpatient OHSS cases–
Aim of inpatient monitoring is to look for changes in the severity of the disease AND to identify any complications at an early stage.
Daily measurement of – Body weight, abdominal girth and fluid intake and output.
Daily labs– full blood count, haematocrit, serum electrolytes, osmolality and liver function tests.
CRP may have a role in monitoring severity ( has been found to correlate with Abdominal girth and weight) .
Other tests may be needed depending on clinical situation- ABG, ECG, Xray chest.
Signs of recovery– Reduction in abdominal girth and body weight.
– diuresis, normalisation of haematocrit
Signs of worsening-Increasing abdominal girth and /or weight
– oliguria with positive fluid balance ; elevated haematocrit .
Management of symptoms of OHSS-
1 . Abdominal pain- Paracetamol, oral opiates ( avoid NSAIDs) . Severe pain warrants evaluation because it may be due to ovarian torsion/ovarian rupture/ ectopic pregnancy/PID.
2. Nausea/ vomiting- antiemetics
Management of fluid balance-
1. Oral fluids- guided by oral thirst.
2. If acute dehydration- i.v fluids( to correct dehydration) , followed by oral fluids ( to maintain hydration) .
3. Colloids- Hexaethyl starch is not available in UK .
Human albumin solution – 25% , 50–100 g, infused over 4 hours and repeated 4- to 12-hours
( Strict fluid balance recording should be followed for these patients)
4. Persistent haemoconcentration or low urine output despite apparent adequate volume replacementà Seek MDT review. Continuous urine output measurement and invasive haemodynamic monitoring may be needed.
5. Oliguria despite adequate fluid – may respond to paracentesis. Diuretics are usually avoided- but may have a role in multidisciplinary setting, if oliguria persists despite fluid replacement and paracentesis. (Stepwise management of oliguria in OHSS– check fluid balance–> paracentesis–> diuretic after MDT review)
PARACENTESIS
– early drainage of ascites to lower the intra-abdominal pressure in
patients with moderate to severe OHSS may prevent disease progression and lower the risk of
severe complications associated with OHSS.
-Usually well tolerated in OHSS patients( because OHSS patients belong to a younger age group)
– Should be done under ultrasound guidance ( To avoid damage to ovaries which are enlarged in OHSS) . Can be done as outpatient also as mentioned above). Can be done transabdominally( This way, an indwelling catheter can be placed- facilitating repeated paracentesis if needed) or Transvaginal ( Usually suitable for single sitting of paracentesis) .
THROMBOPROPHYLAXIS IN OHSS
– Severe or Critical OHSS requiring hospital admission should receive LMWH.
– In Moderate OHSS- Evaluate for other risk factors- prescribe Anti-embolism stockings and LMWH if indicated.
– In women with severe OHSS who conceive, thromboprophylaxis should be considered at least until the end of the first trimester.
– If LMWH is contraindicated in any patient, and she is admitted to hospital with OHSS- her mobility is likely to be reduced- anti-embolism stockings should be prescribed.
Severe OHSS is a prothrombotic state due to haemoconcentration and vascular endothelial dysfunction .
The risk of VTE in IVF pregnancies that have OHSS is increased.
Thrombosis in women with OHSS frequently affects upper body sites and frequently involves the arterial system- therefore may present with unusual symptoms– like dizziness, loss of vision and neck pain. ( Which other conditions are associated with arterial thromboses? *) .
Thromboembolism may occur several weeks after apparent resolution of OHSS, and can occur particularly if there is a pregnancy. The majority of delayed thromboses are reported to have occurred in the first trimester of pregnancy. The GTG Guideline on Prevention of VTE ( GTG 37 a) mentions that in pregnant women with OHSS, thromboprophylaxis should be given at least until the end of the first trimester. The GTG 5 restricts this to women with severe OHSS who conceive ( i.e the OHSS may have occur before the pregnancy is detected).
If thrombosis is suspected- Start therapeutic anticoagulation while imaging is arranged- Collaborate with Maternal medicine and Haematology.
SURGERY IN OHSS- Surgery is only indicated if there is a coincident problem ( like adnexal torsion, ovarian rupture , ectopic pregnancy)
The risk of ovarian torsion or rupture appears to be increased in women with OHSS, particularly in the presence of pregnancy.
Surgery should be performed by an experienced surgeon- ( The ovaries are likely to be highly vascular) . While proceeding for surgery be mindful of the presence of ascitis and enlarged hypervascular ovaries.
Termination of pregnancy is not a recommended treatment option, and has been reported in some rare critical cases only.
–
PREGNANCY AND OHSS-
The risk of miscarriage in pregnancies arising from assisted reproduction cycles complicated by OHSS compared to cycles without OHSS is NOT INCREASED.
Pregnancies complicated by OHSS may be at increased risk of pre-eclampsia and preterm delivery. This should be informed to the woman.
Bonus fact- *Anti phospholipid antibody syndrome can also cause arterial thromboses in addition to venous thromboses.
Disclaimer- This is only a suggested management plan. The content displayed here is for information only. It is not a guideline, and does not replace the Clinical practice guideline of any institution. Optimal clinical discretion should be used in any clinical scenario. Obgresource.com is not responsible for errors or omissions in reporting or explanations. No individual should rely solely on this information to use self -diagnose or self treat any health condition, nor should any individual rely solely on this information to treat any health condition. Obgresource.com cannot provide any assurance or warranty regarding the accuracy, timeliness or applicability of the content. Any external links which are followed are done at your sole responsibility. Utmost clinical discretion is advised in dealing with any clinical situation.
The original guideline can be found here- https://www.rcog.org.uk/globalassets/documents/guidelines/green-top-guidelines/gtg_5_ohss.pdf
The patient information leaflet link is https://www.rcog.org.uk/en/patients/patient-leaflets/ovarian-hyperstimulation-syndrome/