
Author- Dr. Ria Malik ( MD, DNB)
( For clarity, the guideline summary has been divided into two parts
1. Pregnancy with Pre-existing Diabetes and 2. Gestational Diabetes
To Read about Pre-existing Diabetes in Pregnancy- Click here
The NICE recommends testing for GDM for only high risk groups.
- GESTATIONAL DIABETES MELLITUS
RISK FACTORS
Test these groups for GDM( at 24- 28 weeks)
- BMI above 30 kg/m2
- previous macrosomic baby weighing 4.5 kg or above
- previous gestational diabetes
- family history of diabetes (first-degree relative with diabetes)
- minority ethnic family origin with a high prevalence of diabetes.
Prior GDM : Offer early self-monitoring of blood glucose OR
75 gram OGTT in first trimester– If it is normal — > repeat at 24-28 wks
GLYCOSURIA : more than 2+ on one occasions or more than 1+ on 2 occasions :Consider testing for GDM.
Test for GDM 75 gm OGTT, 2hr
Diagnosis if fasting = or > 5.6mmol/L (more than or equal to)
2 hr = or > 7.8 mmol/L (more than or equal to)
( Mnemonic 5678 — 5.6 and 7.8)
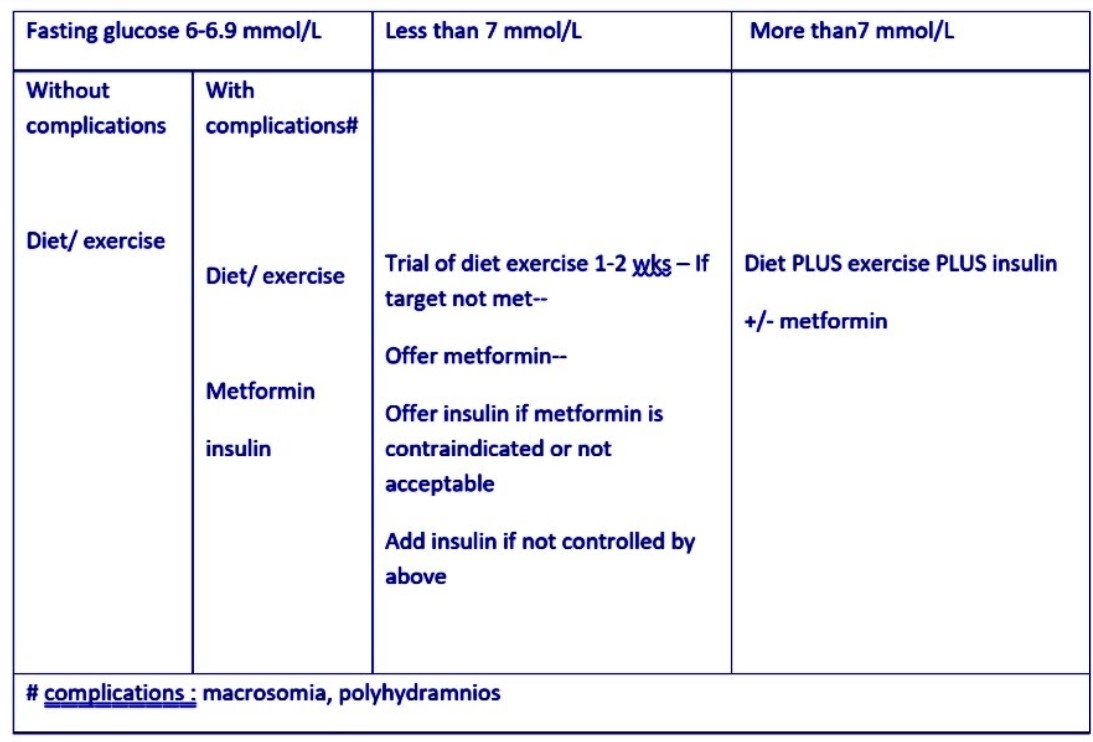
If diagnosed with GDM-
- Check HbA1c ( to detect pre-existing type 2 DM)
- Joint clinic within 1 wk
- Inform the primary team
- Explain to woman the implications, treatment, benefits of control
- Teach self monitoring
- Advise on diet/ lifestyle
- Refer to dietician
Antenatal Care-
Counseling- if gestational diabetes is not detected and controlled, there is a small increase in the risk of serious adverse birth complications such as shoulder dystocia
-Women with gestational diabetes will need more monitoring, and may need more interventions during pregnancy and labour. Some women are able to control the blood glucose with diet and exercise. Most will need oral blood glucose-lowering agents or insulin.
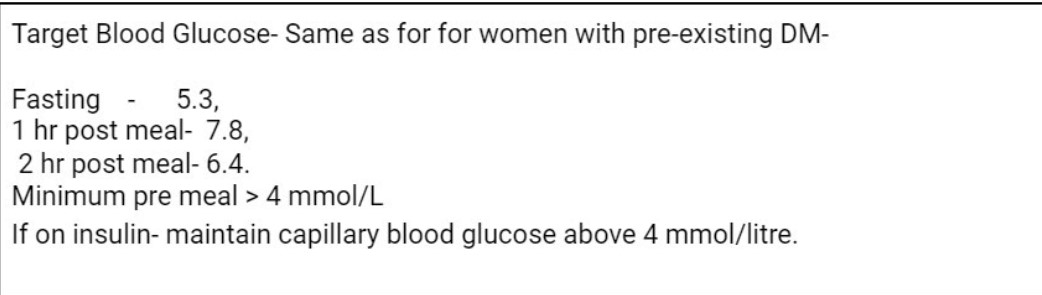
Monitoring blood glucose levels-
- GDM on multiple daily insulin injection regimen – to test fasting, pre-meal, 1-hour post-meal and bedtime blood glucose levels daily.( Same as DM type 1 or DM type 2 on multiple insulin)
- GDM ( or type 2 DM) – managing their diabetes with diet and exercise changes alone or
OR taking oral therapy (with or without diet and exercise changes) or single-dose intermediate-acting or long-acting insulin.- test their fasting and 1-hour post-meal blood glucose levels daily .
Advise to seek urgent medical advice if they become hyperglycaemic or unwell.
Test urgently for ketonaemia if a pregnant woman with any form of diabetes presents with hyperglycaemia or is unwell.
Immediately admit pregnant women with suspected diabetic ketoacidosis for level 2 critical care.
Glibenclamide has been discontinued.
Metformin use in pregnancy for Diabetes is an ‘off label use’
DELIVERY by 40 wks 6 days if no complications.
If complications- deliver before 40 weeks plus 6 days. ( In pre-existing DM without complications- it is 37 to 38 wk 6 days
Delivery in Consultant led unit( neonatal resuscitation skills should be available 24 hours) .
If Obesity and neuropathy : for anesthetist review in third trimester ( Same as pre-existing DM)
BLOOD SUGAR MONITORING IN LABOR (same as for women with pre-existing DM)
In labor : HOURLY (maintain between 4-7 mmol/L, may need Dextrose insulin drip ).
Consider Dextrose insulin drip from start of labor in type 1 diabetes
If general anesthesia: blood sugar monitoring every 30 min from induction of labor to regaining consciousness.
AFTER DELIVERY – stop oral hypoglycemic/ insulin .
POST NATAL CARE–
Test their blood glucose to exclude persisting hyperglycaemia.
If Blood glucose is normal- Offer lifestyle advice, and Follow up for fasting plasma glucose at 6 to 13 weeks.
FOLLOW UP
Remind her about signs/ symptoms of hyperglycemia .
Explain the risks of developing GDM in future pregnancies .
Test blood sugar before planning next pregnancy .
If blood glucose is normal after birth, do Fasting Blood Glucose 6-13 wks OR Fasting plasma glucose/ Hb A1c after 13 wks .
Do not routinely offer a 75- Gram 2 – hour OGTT.
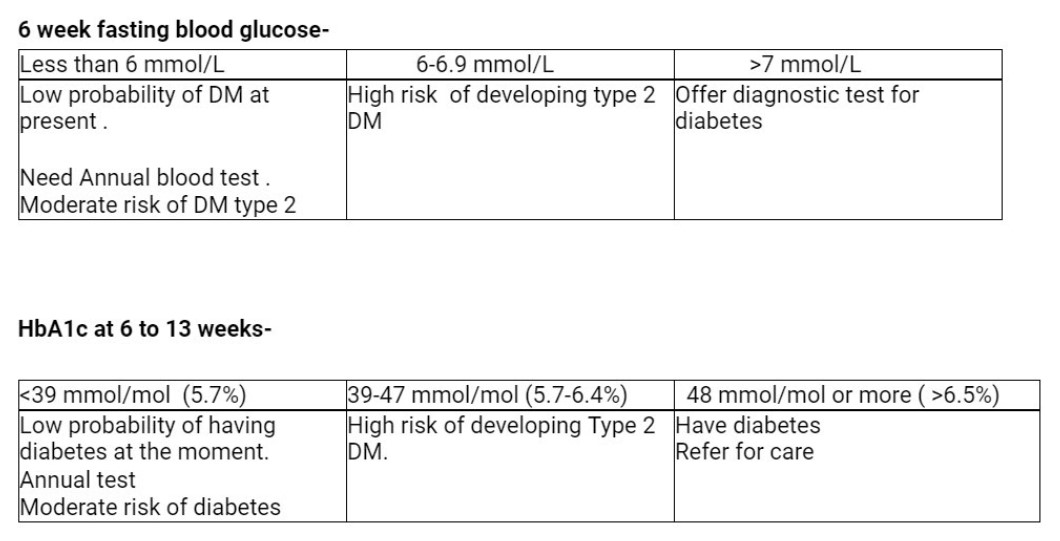
If the postnatal test for diabetes is negative in a woman who was diagnosed with GDM-
Offer annual HbA1c test.
To Read about Pre-existing Diabetes in Pregnancy- Click here
Feedback ? Click here